
Financing Mental Health in Nigeria (2021–2025): Budgetary Trends, Comparative Evidence, and Reform Pathways
Article Sidebar
Main Article Content
Abstract
Background: Mental health accounts for an estimated 14% of the global disease burden yet receives less than 2% of health budgets in most countries, with even lower investment in low- and middle-income settings. This study examines federal mental health financing trends from 2021-2025 to assess whether legislative reform translated into fiscal prioritization.
Methods: A mixed-methods policy analysis was conducted, combining quantitative analysis of federal budget appropriation documents (2021-2025) with qualitative documentary review and comparative case studies. Mental health allocations were assessed by recurrent and capital expenditure, institutional distribution, and proportional share of total federal health spending. WHO reports, national policy documents from Ghana and Kenya, and peer-reviewed literature informed comparative analysis.
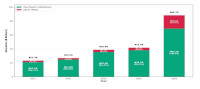
Results: Federal mental health allocations increased from ₦23.33 billion in 2021 to ₦88.24 billion in 2025, a 278% nominal rise. However, the sector’s share of the total health budget declined from 3.67% to 3.12%, indicating relative marginalization. Over 90% of funding supported recurrent expenditures in ten federal neuropsychiatric hospitals, with minimal investment in community-based services or primary care integration. In contrast, Ghana and Kenya more effectively leveraged legislation, fiscal decentralization, and insurance mechanisms to expand access.
Conclusion: Despite legislative reform, Nigeria’s mental health financing remains centralized, hospital-focused, and misaligned with population needs. Institutional inertia, weak coordination, and delayed implementation of the Act have constrained equitable scale-up. Activating the Mental Health Fund and integrating mental health into national financing mechanisms are urgently required to prevent deepening inequities.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
The Journal is owned, published and copyrighted by the Nigerian Medical Association, River state Branch. The copyright of papers published are vested in the journal and the publisher. In line with our open access policy and the Creative Commons Attribution License policy authors are allowed to share their work with an acknowledgement of the work's authorship and initial publication in this journal.
This is an open access journal which means that all content is freely available without charge to the user or his/her institution. Users are allowed to read, download, copy, distribute, print, search, or link to the full texts of the articles in this journal without asking prior permission from the publisher or the author.
The use of general descriptive names, trade names, trademarks, and so forth in this publication, even if not specifically identified, does not imply that these names are not protected by the relevant laws and regulations. While the advice and information in this journal are believed to be true and accurate on the date of its going to press, neither the authors, the editors, nor the publisher can accept any legal responsibility for any errors or omissions that may be made. The publisher makes no warranty, express or implied, with respect to the material contained herein.
TNHJ also supports open access archiving of articles published in the journal after three months of publication. Authors are permitted and encouraged to post their work online (e.g, in institutional repositories or on their website) within the stated period, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See The Effect of Open Access). All requests for permission for open access archiving outside this period should be sent to the editor via email to editor@tnhjph.com.
How to Cite
References
1.World Health Organization. Guidance on community mental health services: promoting person-centred and rights-based approaches. Geneva: WHO; 2021.
2.Gureje O, Abdulmalik J, Kola L, Musa E, Yasamy MT, Adebayo K. Integrating mental health into primary care in Nigeria: report of a demonstration project using the mental health gap action programme intervention guide. BMC Health Serv Res. 2015;15:242.
3.Tandon A, Cashin C. Assessing public expenditure on health from a fiscal space perspective. Washington, DC: World Bank; 2010.
4.Pierson P. Increasing returns, path dependence, and the study of politics. Am Polit Sci Rev. 2000;94(2):251-67.
5.Akyeampong E, Hill AG, Kleinman A, editors. The culture of mental illness and psychiatric practice in Africa. Bloomington: Indiana University Press; 2015.
6.Gureje O, Lasebikan VO. Use of mental health services in a developing country: results from the Nigerian survey of mental health and well-being. Soc Psychiatry Psychiatr Epidemiol. 2006;41(1):44-9.
7.Onwujekwe O, Agwu P, Orjiakor C, Mbachu C, Etiaba E, Ezumah N, et al. Corruption in Anglophone West Africa health systems: a systematic review of its different variants and the factors that sustain them. Health Policy Plan. 2019;34(2):121-35.
8.Abdulmalik J, Kola L, Fadahunsi W, Adebayo K, Yasamy MT, Musa E, et al. Country contextualization of the mental health gap action programme intervention guide: a case study from Nigeria. PLoS Med. 2019;16(8): e1002988.
9.Essien NL. Financial risk protection and Nigeria's journey towards universal health coverage. NPJ Health Syst. 2025; 2:17.
10.Roberts M, Mogan C, Asare JB. An overview of Ghana’s mental health act 2012 (act 846): sharing lessons of implementation. BJPsych Int. 2020;17(4):81-3.
11.Kiima D, Jenkins R. Mental health policy in Kenya-an integrated approach to scaling up equitable care for poor populations. Int J Ment Health Syst. 2010; 4:19.
12.Chisholm D, Sweeny K, Sheehan P, Rasmussen B, Smit F, Cuijpers P, et al. Scaling-up treatment of depression and anxiety: a global return on investment analysis. Lancet Psychiatry. 2016;3(5):415-24.